
Value-based healthcare is a healthcare delivery model where healthcare providers are paid based on patient health outcomes instead of based on the volume of patients seen and services delivered. An additional component of payment is based on the complexity of the patient population for which each provider provides healthcare services. Cost/utilization is greatly impacted by a patient’s annual complexity account, but providers are only paid when the payers understand their patient’s true complexity. Risk adjustment and HCC coding is a major contributor to communicating the true complexity of a patient cohort.
Risk Adjustment and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997, originally created to estimate future costs for a patient. It was only implemented in 2004 and was designed to identify patients with serious or chronic illness and assign a risk factor score to the person based upon a combination of a patient’s health conditions and demographic details. As healthcare shifts towards more value-based payment models; HCC coding is becoming more prevalent of a topic.
To better understand HCC coding, lets first break down Risk Adjustment Factor. Risk Adjustment Factor or RAF uses a patient’s demographics and diagnosis to determine that patients risk score. This score measures how costly a patient is predicted to be for the current year. Within this payment model, patients in the same practice could have a different payment rate. The risk assessment data used is based off claims and medical records collected from doctors’ offices, in-patient hospital visits and outpatient clinics. A multitude of factors determine the amount of risk and work involved to maintain the health of a patient. A patients RAF score is heavily weighted on HCC’s.
So, what are HCC’s? Medicare uses HCCs to reimburse Medicare Advantage plans based on their current member’s health. HCCs are diseases or conditions organized into body systems or comparable disease processes that Medicare correlated with increased cost of care. Out of 72,616 ICD-10-CM codes CMS identified 9,700 diagnosis associated with higher-than-average costs and then assigned them into 86 disease categories. Each of the 86 categories is then placed into a hierarchy of risk. The specific HCC category to which a diagnosis is assigned determines its contribution to the RAF calculation.
The top HCC categories include:
Specificity is key when it comes to HCC coding and documentation. A provider must report on each patient’s risk adjustment diagnosis and it must be based on clinical documentation from a face-to-face encounter. For HCC coding to be successful, the doctor can accomplish documentation standards by using MEAT. MEAT is an acronym used in HCC coding to ensure the most accurate information is being documented for a patient:
M-Monitor signs and symptoms (disease process)
E-Evaluate (test results, meds, patient response to treatment)
A-Assess (ordering tests, patient education, review records, counseling patient and family)
T-Treat (meds, therapies, procedure, modality)
A lot of the work for HCC falls to the coders, to ensure that each patient’s medical record is coded accurately and that there is the supporting documentation regarding the status of the condition. As a certified professional coder, who received certification right at the transition point from ICD-9 to ICD-10, the goal has always been to code to the highest level of specificity. It’s essential to the success of the Risk Adjustment program. While most doctors document reasonably well for medical care, many are unaware of the details needed for accurate code selection for billing, reimbursement, and quality measure purposes. Since most of the burden in documenting for RAF scores is up to the provider, implementing programs within your practice or health care organization such as a Clinical Documentation Improvement (CDI) Program can help bridge that gap between provider and HCC coding.
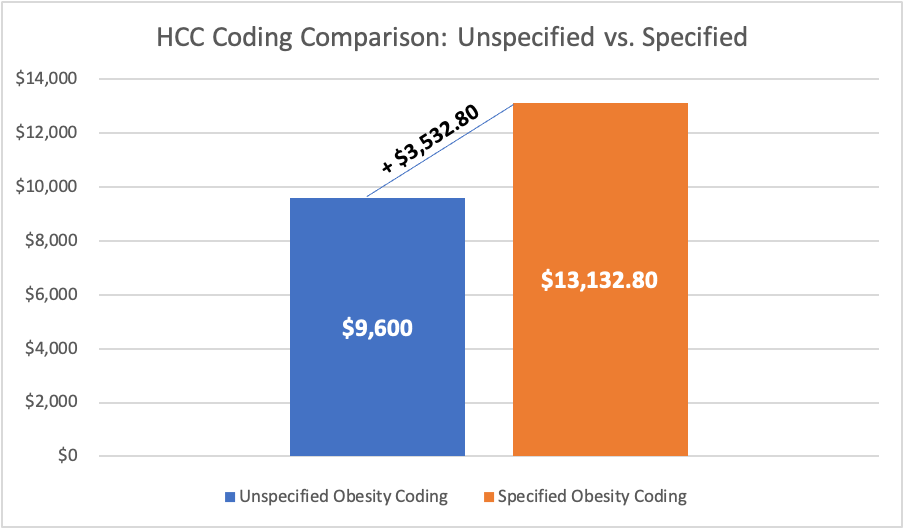
A single patient example helps to convey how critical it is to ensure accurate coding for patients. A female with a weight of 240 lbs. resulting in a BMI of 44 is diagnosed with obesity using ICD-10 code E66.9. This unspecific obesity diagnosis code for this patient has no HCC relevance, which means the patient’s RAF score remains at .000 and payers are unaware of the risk this patient’s weight has on her health and potential cost of care. The more precise and accurate coding of morbid obesity using the E66.01 Dx code would result in a RAF score of .368 for that patient. Figure 1 demonstrates the financial result of more accurate coding for this (normally $800 per member per month costing) patient based only on the addition of a more precise diagnosis coding.
So again, why is HCC coding so important? HCC coding helps communicate patient complexity and paint a picture of the whole patient. In addition, it helps predict healthcare cost utilization. The financial impact of optimizing HCC coding is significant as it directly impacts the money received by a healthcare organization from the largest single payer in healthcare, CMS. Mid-size organizations have been known to lose millions of dollars because of low HCC confirmation rates. Correctly coding HCCs predicts the future financial resources for patients and ensures appropriate reimbursement for physicians…which is always good for your revenue cycle performance. HCC coding is kind of a big deal.