
Let’s examine why the 2019 adjustments are lower than expected
The 2019 MIPS final feedback has been released and adjustments are lower than expected, even lower than expected with COVID-19 already factored into the anticipated results. MIPS eligible practices and clinicians were eagerly anticipating final adjustment rates up to an estimated 4.7%, based on information from CMS. Those estimates were clearly unsuspecting of what a global pandemic can do to shatter the progress being made toward a more Value-Based Care (VBC) centric healthcare model. In order to understand the likely causes of lower-than-expected MIPS payment adjustment rates, it’s important to go through the concessions made through the extreme and uncontrollable circumstances policies and the COVID-19 interim rule-making to account for the pandemic.
The Medicare Quality Payment Program Interim Final Rule Regarding the Extreme and Uncontrollable Circumstance Policy [1] was released to provide flexibilities for clinicians in case of natural disaster. This policy allowed for a CMS response to be issued regarding the COVID-19 pandemic and flexibilities for the 2019 performance period. Here are a few of the main flexibilities regarding MIPS as a result of the CMS response:
- MIPS eligible individual clinicians unable to report anything for the 2019 performance period would automatically avoid MIPS penalties due to extreme and uncontrollable circumstances
- MIPS eligible individual clinicians who reported a single MIPS category would automatically receive a neutral payment adjustment
- For MIPS eligible groups experiencing difficulties or hardship due to COVID-19 preparation and care delivery, CMS reopened the 2019 extreme and uncontrollable circumstance application in 2020 for the month of April. This allowed groups an additional window to submit an application to have MIPS categories reweighted to 0%, therefore avoiding threat of penalty for 2019 (payment year 2021)
Each of the above listed flexibilities set back any chance of a decent MIPS incentive rate. The following details the respective result of each hardship allowance:
- Any individual MIPS eligible clinician, who would have otherwise been penalized for not reporting, avoided penalty decreasing the amount of penalty money in the “pot” to pay out in incentives to higher scoring MIPS clinicians/groups
- Any individual MIPS eligible clinician, who might have only reported on a single MIPS category resulting in a score below the performance threshold, who would have otherwise been penalized for not reaching the threshold, was given a neutral payment adjustment. This avoided penalty also decreased the amount of penalty money in the “pot” to pay out in incentives to higher scoring MIPS clinicians/groups
- MIPS eligible groups experiencing hardship under COVID-19 who submitted a hardship application to avoid penalty, also decreased the amount of penalty money in the “pot” to pay out in incentives
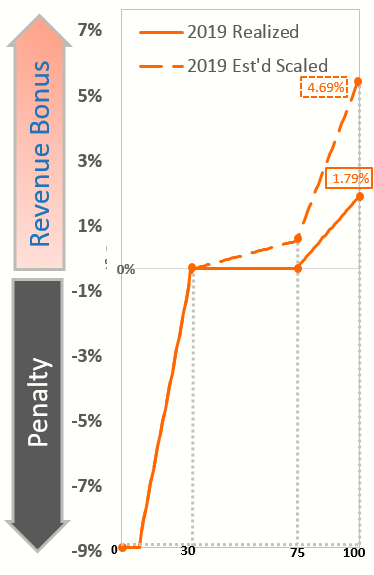
When CMS released the above flexibilities, ReportingMD immediately suspected that the MIPS budget-neutral payment adjustment would not pay any incentives due to the COVID-19 allowances and ReportingMD was correct. The only relief to this assumption was that the MIPS exceptional performance payment adjustment made up 76% of the originally estimated total MIPS incentive possibility, based on information provided by CMS. 3.58% of the estimated 4.69% estimated incentive (with a perfect MIPS Composite Performance Score (CPS)) was expected for the exceptional performance portion of the total incentive. So, what happened to cause the total possible MIPS exceptional performance incentive rate to be cut in half going from 3.58% to 1.79%, as shown in the 2019 Estimated versus Realized image?
Ultimately, the highest performing MIPS clinicians and groups saturated the top of the possible MIPS incentive possibility. As with each of the previous MIPS years, $500 million is distributed starting with 0.5% additional incentives at the minimum exceptional score of 75 up to 10% at the maximum exceptional score of 100. However, this rate is scaled so that it is equally distributed to the number of MIPS eligible clinicians and groups meeting or exceeding the exceptional performance threshold. If most scored MIPS eligible clinicians and groups achieve the highest range of the exceptional performance scale, then the $500 million is saturated with those who should get the largest amount of incentives. When everyone is perfect, there is less exceptional performance money to pay out, thus resulting in the maximum of 1.79% for the 2019 performance year (2021 payment year).
The disappointment over the COVID-19 PHE’s impact on payment adjustments will not be felt exclusively by MIPS eligible clinicians/practices. This pandemic has already impacted several other Value Based Care models/program and will continue to do so as it gains (or at minimum, maintains) speed into the last quarter of 2020. From a mechanics standpoint, the healthcare system has made resources and flexibilities available to allow for the (sometimes lacking) continuation of care in this country. Unfortunately, at a time when individual caregivers and institutions had finally been taking (albeit small) steps forward in acknowledging and implementing the concept of Value Based Care, COVID-19 has already and will continue to jeopardize that progress.
[1] Automatic Extreme and Uncontrollable Circumstance Policy Interim Final Rule, 82 Fed. Reg. 53568 (November 16, 2017) (to be codified at 42 CFR 414). https://www.federalregister.gov/d/2017-24067