By Molly Minehan

By Molly Minehan
Will the CY 2022 Physician Fee Schedule Final Rule with policies for the Quality Payment Program (QPP) finally require action and perhaps even come through with incentives that QPP participants have long awaited? Yes, although more relative to the Merit-based Incentive Payment System (MIPS) track of the QPP than the Alternative Payment Model (APM) track. When the QPP kicked off in 2017, the plan included a phased approach to increased challenge in reporting and scoring until a point in which all MIPS eligible clinicians and practices were being held responsible for a higher degree of care through improved quality and reduced cost. The CMS “triple aim” was the goal after the QPP’s first few years of development but political backpedaling and a pandemic would move the plan forward one step only to fall back five. What wasn’t expected was the bold approach CMS would take in the 2022 QPP final rule, especially with regard to MIPS policies and participants.
The QPP’s first year was designated as a “transition year” in that several less stringent options were offered to QPP participants allowing them to avoid financial penalties while they chose a pathway under the new Medicare and CHIP Reauthorization Act (MACRA) Value Based Care (VBC) models and their underlying objectives. After the initial transition year, the effort requirements and relative penalties/rewards were expected to grow substantially as the MIPS program years went on. Figure 1 below is the graphical representation of what CMS realistically touted as the expected effort and resulting penalties/rewards (per annual rulemaking scaling factor estimates for incentive rates).
FIGURE – 1
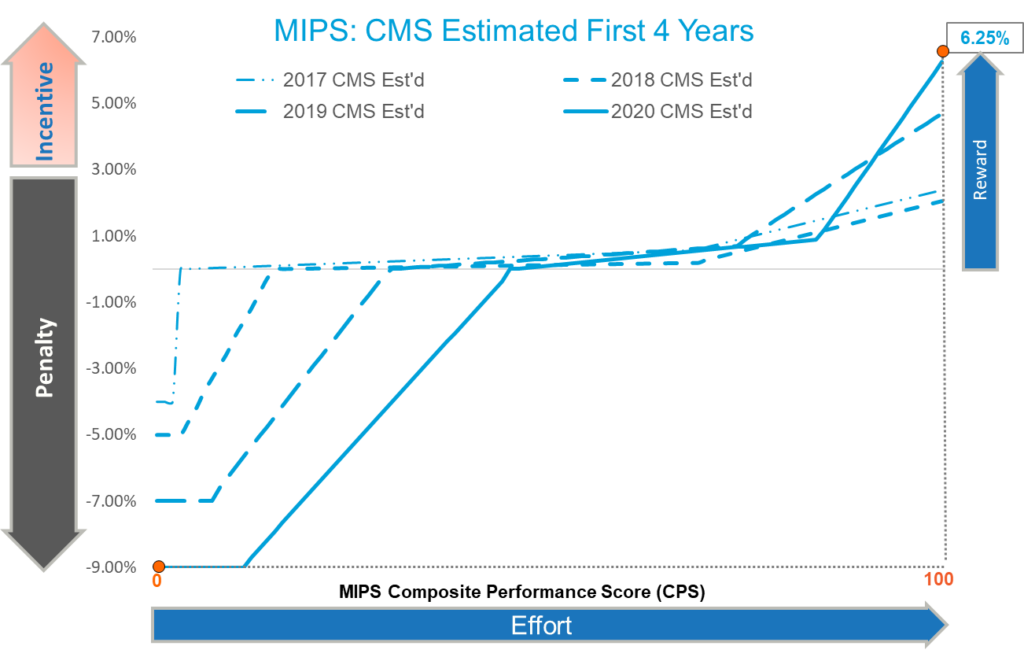
Figure 2 below, however, is the graphical representation of the actual outcome from the first four years of the MIPS program.
FIGURE – 2
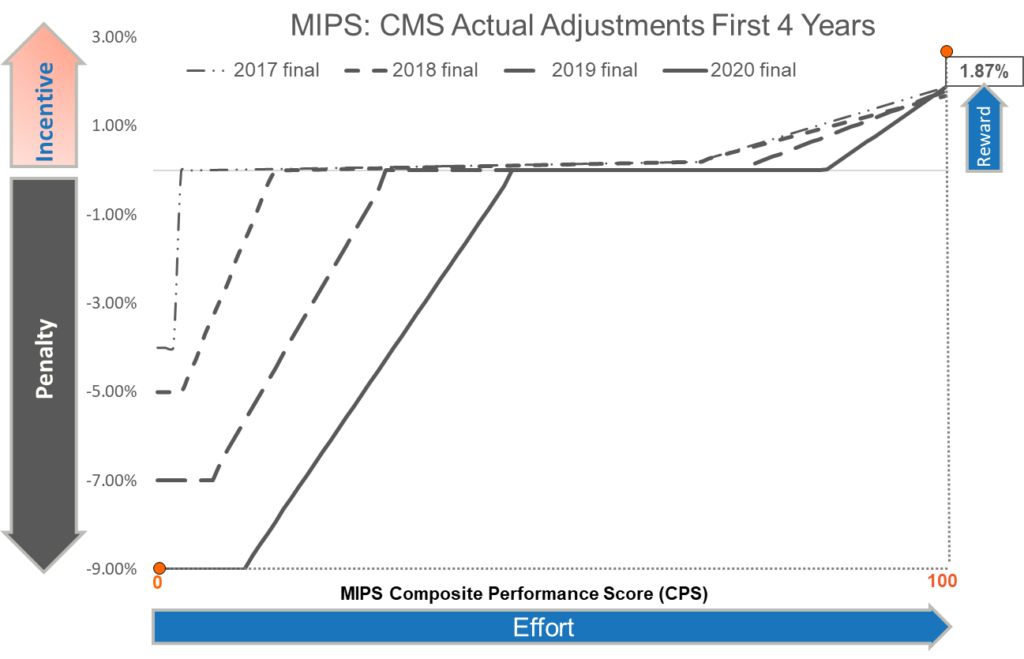
Note (in Figure 1) the max incentive reward of 6.25% with a MIPS score of 100 for 2020 as estimated by CMS in direct conflict with (in Figure 2) the actual incentive reward of 1.87% with a MIPS score of 100 for 2020. This difference of 4.38% in incentives between what CMS advertised for the program and what MIPS eligible clinicians and practices saw as a result of their increased efforts over the first four years of the program, has drawn a significant amount of skepticism toward the program and its ability to meet its goals and objectives.
The story of the Alternative Payment Model (APM) track isn’t all that different from that of MIPS, especially with respect to the Medicare Shared Savings Program (MSSP) Accountable Care Organization (ACO) and it’s changing requirements over the last few annual rulemaking proposals and finalizations. One example was the almost certainty CMS had shown with their proposal to retire the CMS Web Interface as a collection type. This would have effectively required Medicare Shared Savings Program (MSSP) ACOs to move to reporting the MIPS CQMs/eCQMs for 3 active reporting measures as part of the new APM Performance Pathway (APP) instead reporting the ACO measures through CMS WI as they always had done. The slightly under-reported but major impact of this change was that MSSP ACOs would thus be forced to move from reporting on just Medicare beneficiaries to reporting on all payer events for the quality measure reporting requirement. The message was clear in the 2021 proposed and final rules that CMS was forcing the web interface out and didn’t plan to go back on this change. The web interface method was as good as done… or so we thought.
Having been in the CMS “pay-for-reporting” game for over 18 years, ReportingMD knew the switch to all payer patient reporting would be a significant lift. Suddenly, MSSP ACOs would need the ability to aggregate data from various disparate data systems (EHRs, PMs etc) across their various practice participants and report a single set of aggregated measures for the entire ACO. CMS finalized [initially] that the Web Interface collection type would be retired completely in 2022 but could still be used in 2021. ReportingMD made certain that the ACOs were going to be ready for this change coming in 2022 but then in the 2022 proposed and final rules, CMS once again changed their tune. The 2022 rule finalized that CMS would give ACOs until 2025 before they would have to report on all payer events on the 3 MIPS CQMs/eCQM active measures. This gave ACOs an additional 4 years to transition to the increased Shared Savings Program quality performance standard.
When CMS released the 2022 proposed rule and the extensive policy proposals therein, it was met with an appropriate amount of skepticism from several years of rescinded “call to arms”. Fool me once… maybe twice… but not six times! Still in the middle of a pandemic with the Delta Variant running wild, CMS proposed to purge basically every type of MIPS quality bonus point; a luxury MIPS participants have enjoyed for closing quality scoring gaps when performance was lacking. This included end to end bonus points and points for reporting outcome and/or high priority measures beyond the minimum requirement. Additionally, CMS proposed to remove the 3-point floor for quality measure scoring. We had seen this kind of posturing before but still did our due diligence to spread the word to MIPS participants that CMS was proposing policies that would change the program if finalized. We just never thought they would go through with it.
The final rule was released on November 2, 2021 and brought with it good news and bad. The bad news first. Although CMS did not finalize the policy to remove the 3-point quality measure scoring floor for 2022, they did finalize the removal of the end to end and additional outcome/high priority quality bonus points. This finalized policy will decrease MIPS quality scores by up to 20%; even more in cases where other categories are reweighted to quality. So now the good news… MIPS participants that have sought to improve performance across the categories of EHR/PM technology interoperability, quality improvement activities, cost reduction, and quality performance will come out on top in 2022. Those that have worked with experts to understand how best to convey their quality care excellence through sound measure selection for optimal scoring may finally reap the rewards they have been working towards since the start of the program.
Another major change in the 2022 final rule was the increased weight of the Cost category within the MIPS Composite Performance Score (CPS). In 2021, the Cost score was weighted at 20% but there is a legislative requirement to have the Cost category be equal in weight to the Quality category starting with the 2022 performance year. The Cost category does not require any submission as it is calculated by CMS through administrative claims. There are a total of 20 different Cost measures:
The Cost score is the most elusive of the MIPS categories as there is no sure-fire way to improve cost and clinicians subject to its scoring have no control over which measures, they will be scored on. It is solely based on the patients and episodes of care they provide service for and if there are enough to meet the encounter thresholds to get scored on the measure(s). Even though Cost reduction is not directly identifiable, there are ways to reduce cost over time.
As we enter the sixth year of the MIPS program, the Cost category will likely draw more focus and attention as it will be such a large part of the total MIPS score. Work with organizations that can help you target cost reduction efforts and employ the best tactics to reduce cost using a short and long-term approach.
For 2022, CMS has set the performance threshold, that being the minimum MIPS score needed to avoid penalty, at 75 points, which is the highest it has been so far in the program. CMS also finalized that the exceptional performance bonus would be available for the last time in 2022, which was an extension from the original policy that it would only be paid out the first 5 years of the program. To reach the exceptional performance bonus, MIPS participants must reach a total MIPS score of 89 points. That number, without the inclusion of quality bonus points in the MIPS scores and with the elusive Cost category weighted at 30%, will certainly be a challenge to reach but will also be the reason why incentives could be so high from 2022. The numbers are there to back up the realistic possibility that a MIPS participating practice or clinician that reaches a perfect MIPS score of 100 in 2022 may experience a 14.4% upward payment adjustment on all Medicare professional services billed throughout 2024. Figure 3 shows the potential payment adjustment rates covering a MIPS score of 0 up to 100.
FIGURE – 3
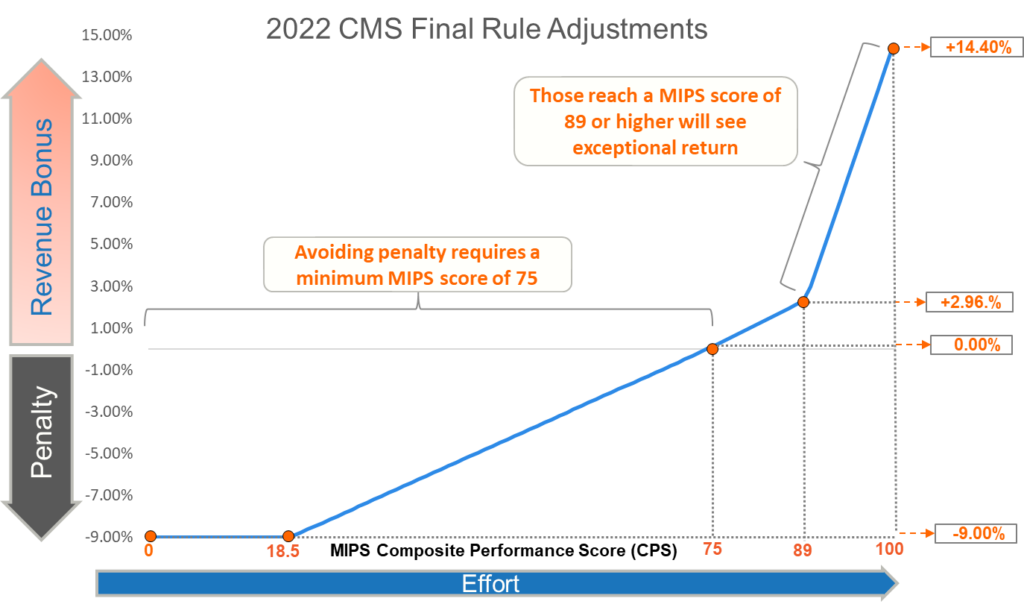
In prior years, the highest MIPS scores saturated the incentive pool so there was less to share because almost everyone had higher scores. For 2022, the prediction is that due to CMS finalized policies on quality bonus points, it will prove far more difficult to reach the performance thresholds the masses have reached in prior years. As a result, there will be more incentive revenue being spread among those few MIPS participants who have stayed the course and prepared themselves for this performance year.
Unfortunately, the common sentiment, which has been expressed more after the final feedback from 2020 than in any year under PQRS, Meaningful Use, or MIPS, is one of complete dissatisfaction with the MIPS program and all it has been advertised to be by CMS officials. ReportingMD experts have continued to support MIPS participants throughout the program and encouraged them to continue their work even when we see their truly impressive MIPS scores go unrewarded and unrecognized. A 10-provider east-coast based Oncology practice reached a perfect MIPS score three of the four MIPS performance years (2017 through 2020). They were just a few points shy of perfection that fourth year. A 400+ primary care practice with an average MIPS score of 97.11 across the 4 MIPS performance years (2017 through 2020). These are the ReportingMD clients that strive to meet the objectives of the triple aim… to improve the quality of care provided to patients, to populations, and to reduce the cost of care in this country. They have done their part and continue to do so. With any hope, the original intentions of the MACRA legislation will begin to manifest as a natural biproduct of the more stringent policies included in the 2022 final rule.