BETTER TOGETHER:
For Providers to achieve optimal performance results for their MIPS quality activities, they need the flexibility, strategy, and insights to leverage both Registry and Electronic Health Record Measures together.
ReportingMD’s Total Outcomes Management (TOM) application is an ONC-certified EHR Technology (CEHRT) module, which allows reporting for both the 45+ electronic Clinical Quality Measures (eCQMs), which are the exact same measures the EHRs offer; and the 175+ registry measures (aka, MIPS CQMs), which registry vendors offer. ReportingMD has been a qualified registry since 2008 and offers practices integration to 50+ EHRs, a cloud-based platform, and dedicated advisors,, and all eCQMs and CQMs to report on. The 25+ measures which have both an eCQM specification as well as a separate and distinct MIPS CQM specification; although they may be similar in nature, these “dual-version” measures are built based on different specifications with different code sets. This dual-version measure option offers a strategic advantage for practices, who can and choose to report on them.
Practices opting to report on dual-version measures essentially get a built-in “2-for-1”. From a clinical data and reporting perspective, since each version of the dual-version measures has different specifications and different code sets, each version can utilize different data to demonstrate the clinical quality actions being done by providers. This is especially valuable to practices in which different providers document in different ways. Each provider does the correct quality actions, but the varying documentation techniques can often result in performance scores not being representative of the true quality of care they provide their patients. In a sense, a lack of standardized and discrete documentation can interfere with performance data delivery resulting in depressed performance metrics.
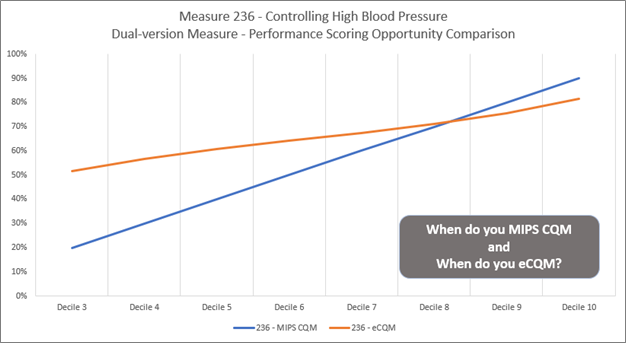
From a performance and scoring perspective, dual-version measures each have their own individual benchmarks. For example, there is a different set of performance deciles for the MIPS CQM (registry) version of measure 236 – Controlling High Blood Pressure and the eCQM version of the same measure (see benchmarks table and image below). Since there are two different benchmark lines for each measure collection method, a practice can benefit by choosing the optimally scored version of the measure even if performance changes throughout the year. For example, if a practice’s performance rate on measure 236 lingers below 60% throughout the year, it would be beneficial for that practice to get scored on the registry version of the measure. If, however, that performance rate changes and goes above 65% then the eCQM would be the better scored. Each version of the measure will have its own performance rate metric and each metric is scored against the individual collection method benchmarks. The question ultimately just becomes, “when do you use MIPS CQM and when do you use eCQM?”
DETAILS MATTER, CQM OR eCQM,:

Offering organizations, the ability to report both versions of dual-version measures to take advantage of the optimal decile scores, means we can help them gain back some lost scoring ground after CMS retired the HP/E2E bonus points. The image below shows an example of a practice that is managing a lot of measures for a variety of specialties:
TOGETHER IN ACTION:
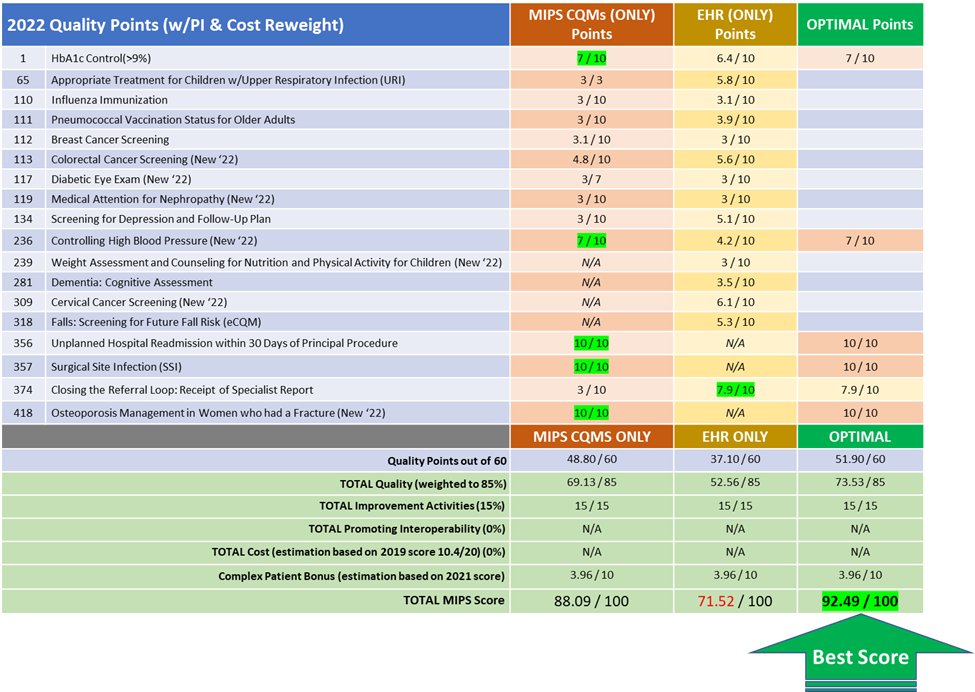
The difference of reporting just registry versus the optimized adds nearly $271,000 in incentive revenue. The difference of reporting just through their EHR versus the optimized is a swing of roughly $450,000 in avoided penalties and MIPS revenue. This practice not only works diligently to improve their quality care, but they do so by investing in their quality infrastructure with resources and systems to help them improve. Each additional MIPS point we can get for this practice, means more quality resources and ultimately better care for their patients.
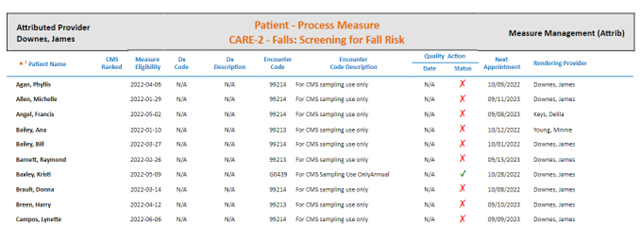
EHR INTEGRATION (PATIENT LEVEL DETAIL):
Integration matters to have the flexibility to leverage both CQMs and eCQMs. Providers need EHR integration to understand at a patient level, where to focus their energies.
GOOD TO GREAT:
As the MIPS program heads into its later years, measure optimization is more important than ever for reporting success and will continue to be for future years. How do practices navigate these uncharted waters? By working closely with ReportingMD experts. Let us help you get the incentive rewards your providers deserve based on the care they deliver.
APPENDIX (MIPS REFRESHER):
Quick review of the MIPS Reporting Year changes: Under standard scoring, the Quality category is lowered to 30% of the overall MIPS score, on parity with Cost (also now 30%) as legislatively required by Congress. Within the Quality category, High Priority, Outcome (HP/O) and End to End (E2E) bonus points are no longer available.
Practices’ MIPS strategic approach for quality category must adjust to absorb the impact of not having HP/O and E2E quality bonus points padding quality scores to close performance and scoring gaps. How will practices ensure their scores meet and exceed the 75-point penalty threshold? The answer is calculated measure selection but also critically important is the ability to report on both versions of the quality measures to reap the scoring advantage of differing benchmarks from the two versions of some measures: Registry measures, often referred to as MIPS Clinical Quality Measures (or, “MIPS CQMs”) and EHR measures, often referred to as electronic Clinical Quality Measures (or, “eCQMs”).